
TL;DR:
- Effective hospital to home care requires early planning, clear communication, and understanding the difference between clinical and non-clinical support. Families should assess needs prior to discharge, reconcile medications, and prepare the home environment to prevent complications and readmissions. Technology and structured support can improve outcomes, but human knowledge and coordinated care remain vital for safe recovery.
Hospital to home care is the coordinated process by which a patient moves from hospital discharge to receiving ongoing support and medical services at home. Families often underestimate how much planning this transition requires. The 30-day period after discharge, commonly called the discharge gap, carries the highest risk of complications and readmission. Understanding the difference between home health care (short-term, clinical, doctor-ordered) and home care (non-clinical, longer-term daily support) is the single most important distinction families need to grasp before their relative leaves hospital. Caremanagers supports families across South Wales and England through exactly this process, matching each person to the right level of care from day one.
What is hospital to home care, and why does it matter?
Hospital to home care is defined as the structured handover of a patient from hospital-based treatment to community or home-based support. The industry term for this process is transitional care, and it covers everything from discharge planning and medication management to arranging nursing visits and daily living assistance at home.

The transition matters because leaving hospital does not mean a person is fully recovered. Clinical oversight drops sharply the moment someone walks through their front door. Without a clear care plan after discharge, gaps in supervision create real danger, particularly for elderly people managing multiple conditions.
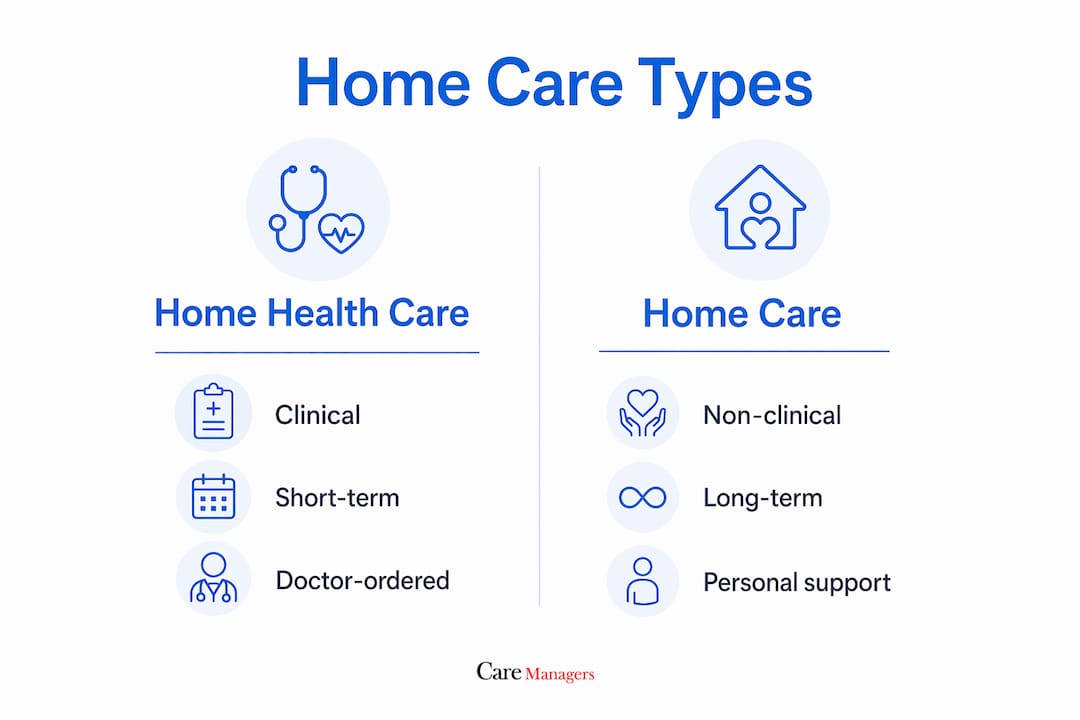
Two distinct service types fill this gap. Home health care delivers clinical services such as wound care, physiotherapy, and medication management. It is short-term, doctor-ordered, and funded through NHS pathways or, in the United States, Medicare. Home care covers non-clinical support: help with washing, dressing, meal preparation, and companionship. It is typically longer-term and often privately funded. Knowing which one your relative needs, and when, shapes every decision that follows.
What are the different types of home care after hospital discharge?
Home care after discharge divides into two clear categories, and families who confuse them often find themselves with the wrong support in place.
Home health care is clinical, time-limited, and prescribed by a doctor. It typically includes:
- Skilled nursing visits for wound care, catheter management, or post-surgical monitoring
- Physiotherapy and occupational therapy to rebuild strength and mobility
- Speech and language therapy following stroke or swallowing difficulties
- Medication administration and monitoring
Home care (also called non-medical or personal care) is longer-term and focuses on daily living. It typically includes:
- Assistance with bathing, dressing, and personal hygiene
- Meal preparation and light household tasks
- Companionship and social support
- Medication prompting (not administration)
The cost difference is significant. Non-medical home care costs around £35 per hour on average, varying by region and provider. Home health care funded through NHS continuing healthcare or a personal health budget may be free at the point of use, depending on eligibility.
| Feature | Home health care | Home care |
|---|---|---|
| Type of support | Clinical | Non-clinical |
| Duration | Short-term | Longer-term |
| Ordered by | Doctor or hospital | Family or individual |
| Typical funding | NHS, insurance | Private pay, local authority |
| Examples | Nursing, therapy | Personal care, companionship |
Most people returning home after a hospital stay need both types, at least initially. Home health care addresses the clinical recovery. Home care fills the daily living gaps that clinical visits leave uncovered.
Why is the transition from hospital to home a critical period?
The discharge gap is the most dangerous phase of a patient’s recovery. Nearly 1 in 5 Medicare patients are readmitted within 30 days of discharge due to gaps in care. The financial cost of preventable readmissions exceeds $26 billion annually in the US alone. That figure reflects a systemic failure to bridge clinical care and home support effectively.
Medication errors are the leading culprit. Medication errors during transitions contribute to up to 25% of hospital readmissions. Medication reconciliation, the process of checking that a patient’s home medications match what was prescribed in hospital, is the single most impactful intervention families and care teams can make post-discharge.
Falls are the second major risk. Elderly people returning home often face an environment that has not been assessed for their changed mobility. A bathroom without grab rails, a loose rug, or a poorly lit hallway can undo weeks of clinical progress in seconds.
Common warning signs families should watch for include:
- Sudden confusion or disorientation
- Fever above 38°C or unexplained chills
- Increased pain or swelling at a wound site
- Shortness of breath or chest tightness
- Refusal to eat or drink over 24 hours
- A fall, even one that appears minor
Pro Tip: Keep a written log of your relative’s symptoms, medications, and any changes in behaviour during the first two weeks at home. This record becomes invaluable when speaking to a GP or district nurse.
Home health care visits typically occur 1–3 times a week for short periods. Without additional private non-medical support, patients risk being unsupervised for most of the day during this critical window. That gap is where complications take hold.
How can families prepare for a safe hospital discharge?
Preparation begins before the patient leaves hospital, not after. Home health care is best arranged before discharge through a hospital assessment that designs a personalised treatment plan involving nursing and therapy. Families who wait until discharge day often find themselves scrambling to fill gaps.
A practical preparation process looks like this:
- Request a discharge assessment early. Ask the ward team or social worker for a formal assessment of your relative’s care needs before a discharge date is set. Dr Tracy Lawrence advises families to request home health assessments proactively to ensure care plans cover nursing and therapy needs.
- Clarify the care plan in writing. Ask for a written discharge summary that lists diagnoses, medications, follow-up appointments, and any restrictions on activity.
- Conduct a home safety assessment. Walk through the home before your relative returns. Remove trip hazards, install grab rails in the bathroom, and check that lighting is adequate in corridors and on stairs.
- Arrange medication reconciliation. Ask the hospital pharmacist to review all medications and provide a clear, up-to-date list. Cross-check this with the GP within 48 hours of discharge.
- Confirm who is responsible for what. Know which nurse or care worker is visiting, on which days, and what they will cover. Identify the gaps and arrange private home care to fill them.
- Set up a communication channel. Kim Entwistle highlights that early transparent communication and symptom monitoring are key to preventing readmissions. Agree on how you will update the care team if your relative’s condition changes.
Pro Tip: Ask the hospital discharge coordinator for a named contact you can call in the first 72 hours after discharge. Most wards have a discharge liaison nurse whose role is exactly this.
Understanding the full home care assessment process before discharge gives families a clearer picture of what support is available and how to access it quickly.
What role does technology play in home care solutions in 2026?
The hospital at home model is the most significant development in post-discharge care in recent years. It delivers acute hospital-level care at home through remote patient monitoring, physician video consultations, and daily nursing visits. Patients receive intravenous medications, diagnostic testing, and clinical oversight without occupying a hospital bed.
The outcomes are compelling. Hospital at home reduces readmissions and costs by 30–38% compared to inpatient stays. Patients also report higher satisfaction and lower rates of hospital-acquired infections. For elderly people in particular, recovering in a familiar environment supports both physical and psychological wellbeing.
The technology underpinning these programmes relies on continuous remote monitoring, AI-based alert filtering, and coordinated dispatch of clinical staff that mirrors hospital workflows from a distance. A CMS waiver valid through 2030 allows reimbursement at inpatient rates for suitable patients in the United States, signalling that this model is here to stay.
The barrier is not technology. Dr Leff emphasises that integrating hospital-level care at home requires payment model shifts and cultural change, and that families should view patient safety as a shared responsibility rather than a clinical task alone. That shift in mindset is as important as any monitoring device.
Pro Tip: If your relative is being considered for a hospital at home programme, ask the clinical team specifically which conditions are being monitored remotely and what the escalation process is if an alert is triggered.
Key takeaways
Safe recovery at home depends on understanding the difference between home health care and home care, closing the discharge gap with continuous support, and preparing thoroughly before the patient leaves hospital.
| Point | Details |
|---|---|
| Know the two care types | Home health care is clinical and short-term; home care is non-clinical and longer-term. |
| Act before discharge | Request a formal assessment and written care plan before your relative leaves hospital. |
| Address medication risk | Medication errors cause up to 25% of readmissions; reconcile all prescriptions within 48 hours. |
| Fill the supervision gap | Clinical visits occur 1–3 times a week; private home care covers the hours in between. |
| View safety as shared | Families, carers, and clinical teams must communicate openly to prevent complications at home. |
What I have learned about families and the discharge gap
The families who manage hospital to home transitions well share one trait: they start asking questions before they feel ready. The ones who struggle tend to wait for the hospital to tell them what happens next. That rarely works.
The discharge gap is real, and it catches people off guard precisely because a patient can look well enough to leave hospital while still being genuinely vulnerable. I have seen families assume that a twice-weekly nursing visit means their relative is covered. It does not. Those visits address clinical tasks. Everything else, the meals, the mobility, the reassurance at 2am, falls to whoever is in the house.
The other thing families consistently underestimate is medication complexity. A person who managed their own tablets for years may return home with a completely different regimen, new doses, new timings, and drugs that interact with things they were already taking. A pharmacist review is not optional. It is the most practical thing a family can do in the first 48 hours.
Technology is changing what is possible, but Dr Leff is right that culture matters more than kit. A monitoring device does not replace a family member who knows their relative well enough to notice that something is off. That human knowledge, combined with good professional care, is what actually keeps people safe.
If you are supporting an elderly relative through discharge right now, the most useful thing you can do is read the why home care matters guidance and then make one phone call to a care coordinator today. Not tomorrow.
— Emm
How Caremanagers supports families after hospital discharge
Caremanagers specialises in post-hospital support for families across South Wales and England, helping to close the gap between clinical discharge and safe recovery at home.
From the moment a discharge date is confirmed, Caremanagers can assess your relative’s needs, match them to the right level of personal care, and put a support plan in place before they arrive home. Whether your family needs a few hours of daily assistance or full live-in care arrangements, the team works around your relative’s preferences and routines. Every care package is built around the individual, not a standard template. To find out what support is available for your family, visit the home care services page or speak to the Caremanagers team directly.
FAQ
What is the difference between home health care and home care?
Home health care is short-term, clinical, and doctor-ordered, covering services like nursing and physiotherapy. Home care is non-clinical, longer-term support for daily living tasks such as washing, dressing, and meal preparation.
How soon should families start planning for discharge?
Planning should begin as soon as a hospital admission occurs. Requesting a discharge assessment early gives families time to arrange home care, conduct a home safety check, and confirm medication changes before the patient leaves hospital.
What causes most hospital readmissions after discharge?
Medication errors contribute to up to 25% of readmissions, with falls and missed follow-up appointments also among the leading causes. Medication reconciliation within 48 hours of discharge is the most effective way to reduce this risk.
What is the hospital at home model?
Hospital at home delivers acute clinical care in a patient’s own home using remote monitoring, video consultations, and nursing visits. It produces readmission and cost reductions of 30–38% compared to inpatient stays, according to current research.
How do I find the right home care after a hospital stay?
Start with a formal needs assessment, either through the hospital discharge team or an independent care provider like Caremanagers. A guide to choosing home care can help families identify the right level of support for their relative’s specific situation.